In today’s society and looking at the community health intervention, community changes as a result of human behaviors can be seen as either a tool or need process. The earlier we understand the important of such a need process the faster we can tackle human behaviors in public health. Several health circumstances begun with behavior threat, such as the real problem of drug abuse, alcohol abuse, excessive tobacco used, irresponsible driving, reckless eating disorder, unprotected sexual attitude and other hasty behaviors that negatively lead to health consequences. There are certain similarities and differences between Transtheoretical model (TM) of change and health belief model (HBM), in terms of chronic disease of colorectal cancer. According to the Nurses’ Health Study (n.d.), the American Cancer Society (ACS) estimates that about 106,680 new cases of colon cancer (49,220 men and 57,460 women) and 41,930 new cases of rectal cancer (23,580 men and 18,350 women) was diagnosed in 2006. Beginning at age 50, men and women who are at average risk of developing colorectal cancer should have a colonoscopy every 10 years.
- Health Belief Model Table:
| Concept | Application |
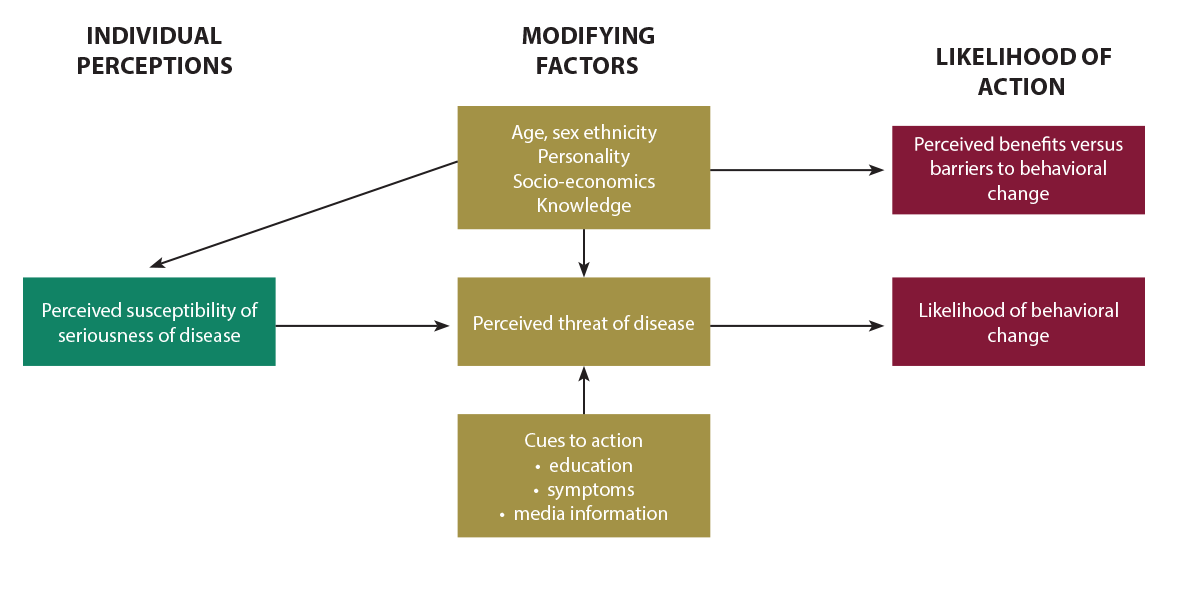
| Perceived Susceptibility | It was well studied and researched to admit that African Americans (AAs) have the maximum degrees of colorectal cancer (CRC) among all races in the US (Lawsin et, al 2007). Persons of such population believed they are exposed to colorectal cancer. |
| Perceived Severity | Colorectal cancer can bring about symptoms such as blood in the stool, dark stool, variations in bowel movements, constipation, diarrhea, or narrow stools. |
| Perceived Benefits | Ways to provide relief and deterrence intervention of colorectal cancer include the changing style of eating, preventing known items of potential to cancer and regular intake of drugs to treat precancerous condition (National Cancer Institute, n.d.) |
| Perceived Barriers | Properly used precautions and prevention procedures of colorectal cancer will lead to happier marriage life, prolonged life happiness and satisfaction. The person of colorectal cancer identified these barriers to eliminating the disease, and to include taking any medications that eradicate the infection. |
| Cues to Action | The person of colorectal cancer have provided inner strategies and willingness to the cue of the disease. |
| Self-Efficacy | The person of colorectal cancer is fully confidence in the provisions of taking actions, using the said strategies. |
- Transtheoretical Model of Change Table:
| Concept | Application |
| Precontemplation (Not Ready) | The person of colorectal cancer is very resilient and unprepared to make changes or get help toward his or her disease. |
| Contemplation (Getting Ready) | The person of colorectal cancer is getting ready with good intentional motive to tackle the disease, usually within 6 months. |
| Preparation (Ready) | The person of colorectal cancer is ready to take immediate actions in tackling the disease within short period of time, usually in the next month or less. |
| Action | The personal of colorectal cancer has taken actions in reducing the disease infection or even eliminating it, usually even six months ago. |
| Maintenance | The personal of colorectal cancer is working in upholding the prevention of revert, usually a period that last six to one year. |
| Termination | The person of colorectal cancer are not tempted to the habitual effect of the disease and fully self-efficacy. |
Colorectal cancer (CRC), also known as bowel cancer, colon cancer, or rectal cancer, is the development of cancer from the colon or rectum (parts of the large intestine). Colorectal cancer is the third most communal cancer in men and women, and the second most communal cause of cancer death in the U.S. — accounting for 147,500 new cases and 57,100 deaths in 2003 (Jemal & Murray, 2003). One of the similarities between the two models in explaining colorectal cancer is that very few theoretically based studies are available to explain the effective screening procedures and behavior pattern of colorectal cancer. That is to say, there are very few research-based models of comportment that can enlighten non-adherence to colorectal cancer screening/methods among low-income or African American population (Lawsin, Duhamel, Weiss, Rakowski, & Jandorf, 2007). Additionally, HBM and TTM are among the basic theories that can far explain the intervention, and prevention approach of colorectal cancer (CRC: Lawsin et al, 2007). It was well studied and researched to admit that African Americans (AAs) have the maximum occurrence of colorectal cancer (CRC) among all races in the US (Lawsin et, al 2007). Achievement of CRC screening is reliant in part on the proportion of uptake by the targeted population like African American (Almadi et al, 2015). HBM was used in the article of Almadi et al (2015) to identify factors that were related to readiness of experiencing CRC screening. TTM and HBM are the two most widely used theories of individual behavior change in public health. This is because both theories are practical, intuitive, and easily applied. Some situations could use both theories — you may find out that both have similarities. Still, there are important differences. One of the differences between the two models is that TTM can explain health issue of colorectal cancer as a way of helping patients make sense of their behavioral change process. TTM has the potential to explain change process in the prevention and precaution of the disease. It is fair to say the behavioral change of individuals and animals has been the central focus of many theorists, such as the founder(s) of HBM and the originator(s) of the TTM. On the same token, TTM is a modern psychological and classical behavioral change employed to initiate efficient interventions and to promote healthy behavioral changes. The study by Lawsin et al (2007) was aimed at furthering the discussion on the similarities of the two models, and by enhancing the understanding of influences associated with CRC screening recommendations, and of stage of adoption for CRS screening among sample of African American population.
One of the influential and classical works I found in the unique use of HBM was the training of Community Health Workers (CHW) in the learned decision-making procedure for prostate screening among African American males. The research proposed a planned curriculum to train CHWs in utilizing HBM theory-driven approach to facilitate IDMs elevation of prostate screening among African American men. ACS (2009) recommended that African Americans experience a 60% higher incidence of prostate cancer, and are twice as likely to die when spotted in comparison to whites. CHWs that are versed in the HBM will be aware of how these variations can effect prostate screening decisions and their uniquely natural role as culturally competent educators. Based on the results of this study, focus group responses were consistent with the HBM model in decision-making. In regard to prostate screening that was built from the current literature, CHWs showed an enhancement in health outreach about prostate cancer, to promote and aid screening IDMs. Examples of ways that provide relief and deterrence intervention of colorectal cancer include healthy lifestyles; preventing known food items that are prone to cancer, and regular intake of precancerous-preventive drugs (National Cancer Institute, n.d.)
Reference
Almadi, M., et al. (2015). Effect of public knowledge, attitudes, and behavior on willingness to undergo colorectal cancer screening using the health belief model. Saudi Journal of Gastroenterology, 21(2), 71-77. doi:http://dx.doi.org/10.4103/1319-3767.153814
American Cancer Society (2009). Cancer Facts & Figures for African Americans 2009-2010. Retrieved from http://www.cancer.org/acs/groups/content/@nho/documents/document/cffaa20092010pdf.pdf
Jemal A, Murray T, Samuels A. (2003). Cancer Statistics. CA Cancer Journal Clinic, 53, 5–26.
Lawsin, C., Duhamel, K., Weiss, A., Rakowski, W., & Jandorf, L. (2007). Colorectal cancer screening among low-income African Americans in east Harlem: A theoretical approach to understanding barriers and promoters to screening. Journal of Urban Health, 84(1), 32-44. doi: http://dx.doi.org/10.1007/s11524-006-9126-6
National Cancer Institute (n.d.). Colorectal Cancer Prevention (PDQ®).
Retrieved from http://www.cancer.gov/types/colorectal/patient/colorectal-prevention-pdq
The Nurses’ Health Study. (n.d.). Findings: Some Facts. Retrieved from http://www.channing.harvard.edu/nhs/?page_id=197
US Center for Disease Control and Prevention (n.d.). National Prevention Strategy. Retrieved March 29, 2015 from http://www.cdc.gov/features/preventionstrategy/








